How Wearable EEG Could Predict Migraines: An Interview with Annemijn Oosterlee

Annemijn S.J.C. Oosterlee is a medical researcher in neurology at the Hoofdpijn Onderzoek team, focusing on the electrophysiological and behavioral characteristics of migraine. Her work aims to map these features to better understand migraine mechanisms and explore possibilities for predicting migraine attacks. She is part of a research team looking into this subject, consisting of Professor Gisela Terwindt, neurologist at the LUMC, Assistant Professor Mark van de Ruit, biomedical engineer at TU Delft, and Jamie Duijvelshoff, a biomedical engineer PhD candidate at TU Delft.
Annemijn holds an MSc in Medicine from Leiden University and collaborates internationally, including as a member of the International Headache Society (IHS). She is a PhD candidate at Leiden University Medical Center (LUMC). Her research combines clinical expertise with cutting-edge neurophysiological methods to advance migraine diagnostics and patient care.
Reading the Brain Before the Pain
To start, could you briefly introduce yourself, outline your research background, and describe how EEG fits into your work?
My name is Annemijn Oosterlee, and I am a third-year PhD candidate at the Department of Neurology at Leiden University Medical Center (LUMC). I am part of a research team together with Professor Gisela Terwindt from the LUMC, assistant professor Mark van de Ruit, and PhD candidate Jamie Duijvelshoff from the TU Delft. Our research focuses on predicting migraine attacks.
To do this, we use EEG measurements collected by patients in their homes to investigate whether changes in cortical excitability occur during the pre-ictal phase of a migraine attack (the 24 hours before the headache phase begins). Our goal is to determine whether these changes serve as early warning signals of an impending migraine attack.
What makes migraine attacks challenging to understand, and why is predicting them a key objective of your work?
Migraine attacks are often unpredictable and can significantly disrupt patients’ daily lives. Being able to predict an attack would reduce this uncertainty and allow patients to plan their lives more easily. With the development of new migraine medications, such as gepants [1] (a class of drugs used for both the acute treatment and prevention of migraine), it is possible to prevent an attack altogether, as these medications can be taken before the onset of the headache phase.
This would enable the use of situational prevention: taking a gepant shortly before an anticipated attack as targeted treatment to prevent that specific episode, rather than relying on a standard oral preventive medication that must be taken daily, often has more adverse effects, and is primarily intended to reduce the overall frequency and intensity of attacks.
Moreover, gepants do not carry the same risk of medication-overuse headache as standard acute treatments, such as analgesics and triptans. Situational prevention, therefore, represents an approach that lies between traditional preventive and acute therapies and is well aligned with ongoing advances in personalized medicine.
Your publication is part of the migraine@home and brain@home monitoring projects. Could you describe the overarching goals of these initiatives and the clinical or scientific gaps they aim to address?
The overarching goal is to apply real-world clinical neurophysiological and neurobehavioral markers as novel human measurement models for personalized treatment of migraine and epilepsy. For migraine, we use EEG recordings to identify changes during the pre-ictal phase (approximately 24 hours before the headache phase). To determine whether a measurement corresponds to the pre-ictal or interictal phase, we rely on our validated E-diary [2], which provides a baseline of each patient’s normal cortical excitability for comparison. Additionally, we use a trigger E-diary that asks patients daily about potential migraine triggers, helping to identify patterns that may precede an attack. Finally, we incorporate tappigraphy data from a smartphone app that records typing speed and patterns, allowing us to detect subtle changes that may occur before a migraine. The app also estimates the user’s location, enabling the integration of weather data into migraine prediction.

The research team: Annemijn Oosterlee, Gisela Terwindt, Mark van de Ruit and Jamie Duijvelshoff
A key element of your work is the shift toward EEG measurements performed by participants at home. From a research and clinical perspective, what makes home-based EEG particularly valuable for migraine research?
This is particularly important because we previously found that the added change of patients having to come to the hospital every day actually delayed migraine attacks. As a result, measurements taken in the hospital are often limited to interictal periods, while pre-ictal measurements, critical for our study, are lacking. Additionally, requiring patients to come to the hospital or for researchers to visit patients’ homes daily created logistical challenges, which led to fewer satisfactory measurements than we had hoped.
When patients measure themselves at home, we believe it provides a more accurate representation of their daily environment and allows for longer monitoring periods, increasing the likelihood of capturing pre-ictal measurements. Moreover, we include only patients who experience at least 1–2 migraine attacks per month, and we have observed that these attacks are more likely to occur when patients self-monitor at home, whereas they occur less frequently in the hospital setting.
One note: this study, which focused on the user-friendliness and usability of our EEG home setup [3], tested healthy participants (we did not record migraine diagnoses), since the primary focus was usability. However, for the portion of the study evaluating the usability of our headache E-diary, we included migraine patients, as they are the intended users of the diary.
In this study, you combined the APEX, our mobile EEG amplifier, with water-based EEG electrodes. What were the main considerations behind selecting this combination for the migraine@home monitoring setup?
How did setup time and ease of use factor into this decision?
When we first began performing at-home EEG measurements, I still prepared the participant and recorded the EEG data myself. Initially, we used the SAGA system together with the Infinity Gel Cap. The gel-based cap offers the gold standard for EEG signal quality. However, it is not suitable for independent use by patients, as we found that they could not reliably apply the gel on their own. In particular, they struggled to apply it correctly to the back of the head, the area most critical for our measurements of the visual cortex. To create a fully self-administered system, we then transitioned to the more compact and mobile APEX EEG amplifier combined with an easier-to-set-up water-based cap.
With the water-based system, users simply wet the sponges, insert them into the cap, and then place the cap on. We found this approach highly user-friendly. In addition, the APEX is very compact, making it easy for patients to use independently.

Infinity water EEG headcap

APEX EEG amplifier
Did the system meet your expectations in terms of signal quality in a home environment?
Patients are able to successfully record an EEG in the home environment. We learned that to achieve this, careful instructions and real-time feedback on the electrode impedance are crucial throughout the application process. We partner with Clinical Science Systems to develop a digital step-by-step software application that guides patients through setting up the EEG recordings and achieving appropriate EEG signal quality when recording independently at home. Our latest setup includes a tablet running their NeuroCenter software, which allows live viewing of measurements and the opportunity to provide help remotely when required.
Your study reports very high compliance rates and usability scores for both the E-diary (electronic headache diary) and the EEG setup. What do these results tell us about the feasibility of self-administered EEG monitoring in real-world settings?
We believe that telemonitoring using a combination of the E-diary and EEG setup is entirely feasible. We are already implementing this approach in our Migraine@Home project, where 25 patients have recorded EEG measurements at home while completing the E-diary daily. This allows us to distinguish which measurements were pre-ictal and which were not. Our goal is to expand the study to include many more patients.
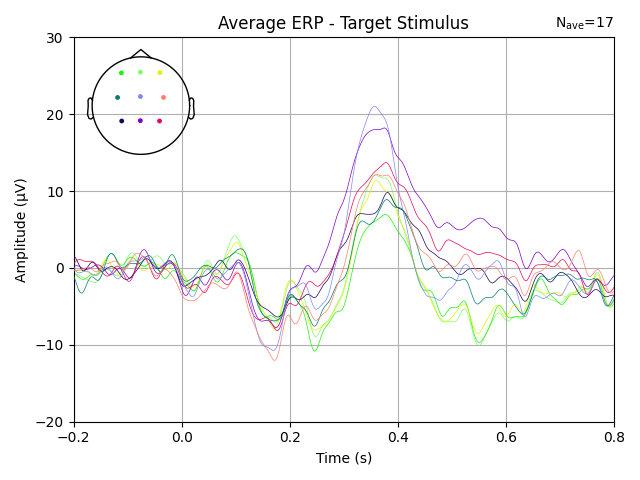
Beyond the EEG system itself, your setup included components such as LED goggles and a trigger box. Could you explain their role within the study protocol and how they contribute to understanding or predicting migraine attacks?
We believe the visual cortex plays a key role in migraine, as it is the origin of cortical spreading depolarization during migraine aura. Therefore, if changes in cortical excitability occur, we expect the highest likelihood of detecting them in the visual cortex. To enhance our chances, we specifically stimulate the visual cortex. This is achieved by providing flashes of light at specific frequencies through LED goggles, while we record the brain’s responses. Our goal is to investigate whether these responses differ in the pre-ictal phase compared to the interictal phase.
Based on your findings, how do you see home-based EEG contributing to the future of migraine care, particularly in terms of prediction, personalization, or treatment evaluation? What would need to happen for this approach to move closer to routine clinical use?
Currently, the EEG setup is used exclusively in a research setting. Our first goal is to confirm, in a larger cohort, that measurable changes in cortical excitability occur during the pre-ictal phase of a migraine attack and that these changes could serve as a predictive warning tool, as we have already demonstrated in a smaller cohort [4]. The next step would be to develop a more portable system that requires minimal electrodes, and measurement time to record EEG, and to explore whether it can be combined with biomarkers from other wearables, such as smartwatches.
Finally, what are the next steps for your research, and how do you see mobile, user-friendly EEG technology shaping future brain monitoring studies?
Our next steps involve identifying these excitability changes in a larger cohort, which requires recruiting many more participants willing to perform self-measurements. Following this, we aim to integrate data from the trigger E-diary and smartphone tappigraphy with the EEG recordings, ultimately creating a single, user-friendly application to predict migraine attacks.
“We thank Annemijn and her research team at LUMC for sharing their insights and expertise on enhancing migraine prevention and overall health.”
References
Lipton RB, Ailani J, Mullin K, et al. Situational prevention: Pharmacotherapy during periods of increased risk for migraine attacks. Headache 2024; 64: 859-864. 20240703. DOI: 10.1111/head.14775.
van Casteren DS, Verhagen IE, de Boer I, et al. E-diary use in clinical headache practice: A prospective observational study. Cephalalgia 2021; 41: 1161-1171. 20210502. DOI: 10.1177/03331024211010306.
Oosterlee A, van der Arend BWH, Duijvelshoff JL, et al. Enhancing migraine care and research through Telemedicine and telemonitoring: E-diary tracking and home EEG. Comput Struct Biotechnol J 2025; 28: 380-385. 20250911. DOI: 10.1016/j.csbj.2025.09.007.
Perenboom MJ, van de Ruit M, Zielman R, et al. Enhanced pre-ictal cortical responsivity in migraine patients assessed by visual chirp stimulation. Cephalalgia 2020; 40: 913-923. 20200318. DOI: 10.1177/0333102420912725.








Migraines affect over one billion people worldwide, yet predicting when the next attack will strike remains one of neurology's unsolved challenges. What if your brain could warn you before the pain begins?
We sat down with Annemijn Oosterlee, PhD candidate at Leiden University Medical Center, who is investigating —alongside her research team— whether wearable EEG technology can detect subtle shifts in brain activity in the hours before a migraine hits, to learn about the science, challenges, and what this could mean for the millions living with migraine.